Scoliosis surgery in children
Web link: Open online
Zotero link: Open in Zotero
Tags: ../../pages/Orthopaedic surgery, Scoliosis,
Abstract
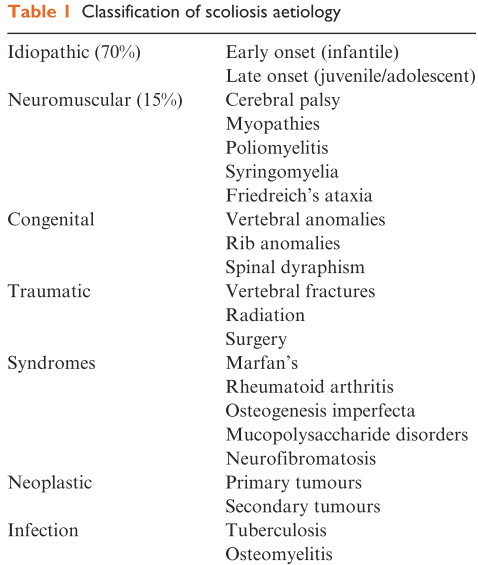
Scoliosis is a lateral curvature and rotation of the thoraco-lumbar vertebrae with a resulting rib cage deformity. It may be idiopathic or secondary to neuromuscular disease, infection, tumour or injury (Table 1). Curvature is measured using the Cobb angle (Fig. 1). A lateral curve of >10° is considered abnormal.1
Notes
Annotations
(8/11/2022, 11:06:57 PM)
“Scoliosis is a lateral curvature and rotation of the thoraco-lumbar vertebrae with a resulting rib cage deformity. It may be idiopathic or secondary to neuromuscular disease, infection, tumour or injury (Table 1). Curvature is measured using the Cobb angle (Fig. 1). A lateral curve of >10° is considered abnormal.” Go to annotation (Entwistle and Patel, 2006, p. 13)
“restrictive lung disease attributable to scoliosis compounds the respiratory weakness associated with neuromuscular disease.” Go to annotation (Entwistle and Patel, 2006, p. 13)
“There is evidence that scoliosis surgery can be well tolerated despite severe restrictive lung disease (FVC < 32%).3 Approximately 25% patients with idiopathic scoliosis have mitral valve prolapse, but this is rarely of clinical significance and antibiotic cover is given.” Go to annotation (Entwistle and Patel, 2006, p. 14)
“Preoperative assessment of patients with neuromuscular disease or immobility is more difficult. They are neither able to give a history of exercise tolerance nor perform spirometry adequately. Muscular dystrophies may be complicated by subclinical cardiomyopathy. More than 50% of patients with Duchenne muscular dystrophy have some degree of dilated cardiomyopathy and an ejection fraction <45% by 15 yr of age. Any reduction in ejection fraction may mean difficulties coping with the rapid fluid shifts during surgery. ../../Knowledge/Medicine/Echocardiography is required to assess left ventricular function in these patients; however, a normal study does not exclude significant pathology.” Go to annotation (Entwistle and Patel, 2006, p. 14)
“succinylcholine is contraindicated in patients with muscular dystrophy because of the risk of rhabdomyolysis, hyperkalaemia and cardiac arrest.” Go to annotation (Entwistle and Patel, 2006, p. 14)
“Postoperative blindness has been attributed to external eye pressure reducing optic nerve and retinal perfusion” Go to annotation (Entwistle and Patel, 2006, p. 14)
“Children with neuromuscular disease are at increased risk of excessive blood loss. They have more osteopenic bone and it has been suggested that the absence of dystrophin causes vascular pathophysiological changes.” Go to annotation (Entwistle and Patel, 2006, p. 15)
“Exposure to allogenic blood transfusions can be reduced by techniques to minimize blood loss. Simple measures include careful positioning to avoid inferior vena cava compression, preventing hypothermia, correction of coagulopathy and good surgical technique. Compression stockings and pneumatic boots are used as thromboprophylaxis, avoiding anticoagulants.” Go to annotation (Entwistle and Patel, 2006, p. 15)
“Controlled hypotension has been shown to reduce blood loss during spinal surgery. Many methods have been described; however, a mean arterial pressure of 50–60 mmHg can be achieved with a remifentanil infusion and volatile agent without the need for vasodilators. Hypotension and surgical manipulation may reduce spinal cord perfusion and so risk neurological injury. It is therefore important to maintain continuous neurological monitoring (see below) and an adequate haematocrit to ensure oxygen delivery.” Go to annotation (Entwistle and Patel, 2006, p. 15)
“Neurological injury may occur because of
- direct spinal cord or nerve damage during instrumentation,
- distraction injury or
- reduced spinal cord perfusion resulting in ischaemia.
Intraoperative spinal cord monitoring is used in an attempt to detect neurological injury and prevent devastating, irreversible damage.” Go to annotation (Entwistle and Patel, 2006, p. 15)
“The nervous system is stimulated and the response is monitored distal to the area of spinal cord at risk. This may be done using somatosensory evoked potential (SSEPs) or motor evoked potential (MEPs). SSEP monitoring involves stimulating a peripheral nerve, often the posterior tibial nerve, and then detecting a response with epidural or scalp electrodes. The evoked potentials are averaged more than 2–3 min to eliminate background noise then displayed as voltage against time. Nerve injury may be indicated by ↓ amplitude or ↑ latency. In MEP monitoring, transcranial electrical impulses stimulate the motor cortex and the resulting signal is detected with epidural electrodes or as compound muscle action potentials (CMAPs).” (Entwistle and Patel, 2006, p. 16)
“Anaesthetic technique impacts upon spinal cord monitoring. Volatile agents, propofol and ../../Knowledge/Medicine/Nitrous oxide all depress SSEPs and MEPs; however, opioid have little effect. ../../Knowledge/Medicine/neuromuscular blocking agent may reduce background noise when using SSEPs, but a profound block will prevent CMAPs. Decreases in blood pressure and temperature may also depress signals. Baseline recordings are made after induction of anaesthesia and a steady state maintained to minimize drug induced changes. Any ↓ amplitude, ↑ latency or loss of waveform must then be attributed to neurological injury. If a change in the recorded evoked potentials occurs and an injury is suspected, a ‘wake-up’ test should be performed.” Go to annotation (Entwistle and Patel, 2006, p. 16)
“The ==‘wake-up’ test ==provides a snapshot of spinal cord motor function. Surgery is halted, the volatile agent switched off and emergence allowed. The patient is asked to move their feet and, once this occurs, anaesthesia can be recommenced. Assistance is needed to prevent patient movement which may cause accidental extubation or loss of vascular cannulae. In the event of new paraplegia, all implants should be removed, hypotension and anaemia corrected, and a course of high dose methylprednisolone commenced.” Go to annotation (Entwistle and Patel, 2006, p. 16)
References to check out
Anaesthetic care for surgical management of adolescent idiopathic scoliosis